Why behavioral data is key to better health and the case for payment models to support its use
The move towards value-based care has awakened the healthcare industry to the importance of the ‘social determinants of health (SDoH)’ – economic stability, education, social community, and physical environment – in shaping health. That’s a great first step because these factors are proving to be more important in determining health than medical care.[1], [2]
While SDoH are important drivers of health, they don’t capture the 30% to 40% of our health that is shaped by our behaviors. Many SDoH factors, such as zip codes or education levels, can’t be readily changed. To really move the needle, we need to layer in data on a population’s attitudes and behaviors – what we call the socio-behavioral determinants of health (SBDoH).
And—this is a crucial point —we need to make sure that our payment models adequately support these efforts. Encouragingly, a recent survey found that eight in 10 payers are incorporating SDoH into their member programs.[3] We urge them to take the next step by incorporating consumer behavioral information to develop programs that help members modify unhealthy behaviors.
Reducing chronic conditions through behavior change
Chronic conditions are the most common, costly, and preventable health issues in the US, accounting for 86% of our health expenditures.[4] About half of all US adults have two or more chronic conditions, and in 2016, each of the top five causes of death were associated with modifiable behaviors such as diet, smoking, and physical inactivity (Figure 1).[5]
To impact these expensive yet preventable health conditions, we need to know what people’s behaviors are, then intervene at the right time, with the right tools to change unhealthy habits.
| Rank | Cause of Death | Behavioral Risk Factors |
| 1 | Heart Disease | Inactivity, smoking, diet |
| 2 | Cancer | Inactivity, smoking, diet |
| 3 | Chronic lower respiratory diseases | Smoking |
| 4 | Accidents | Alcohol use, drug use |
| 5 | Stroke | Uncontrolled blood pressure, diet |
Figure 1: Behaviors Linked to Leading Causes of US Deaths
Adapted from “R.M. Kaplan, S.B., Johnson, P.C. Kobor. “NIH Behavioral and Social Sciences Research Support: 1980-2016” American Psychological Association. 2017. 72(8). 808-821.”
As Gartner observed in 2017, “Health agencies will have to become at least as sophisticated as other consumer/retail industries in analyzing a variety of data that help uncover the root causes of human behavior. The ability to influence behavior will be the key to transforming long-term management of cost and quality outcomes.”[6]
The next step: socio-behavioral determinants
To prevent chronic conditions before onset, we need to harness data about people’s behaviors and attitudes as well as their SDoH. Data such as fast-food habits, tobacco use, physical activity, beliefs about diet, alcohol/drug use, stress levels, social isolation, and media habits, gives providers critical insights into patients’ lives as well as the best ways to engage them. This allows providers to deliver more customized visits and greater value for each unique patient.[7] SBDoH is a next step in the transition to value-based care, and perhaps the missing piece to accelerate positive outcomes.

Figure 2: Behaviors are more amenable to change than SDoH factors
Using SBDoH to impact diabetes
Diabetes is a useful example of a chronic disease that can be managed beyond medical intervention, through behavioral changes. The right reimbursement approach can support a population health strategy that leverages team-based care, self-management tools, and community support partners. To successfully battle a disease like diabetes, you need:
- A PHM platform that aggregates and normalizes data from a variety of sources, establishes a robust diabetes registry, identifies high-risk patients and patients who aren’t being seen, and benchmarks individual/clinical/national progress points[8]
- The right team of providers and community partners
- Mechanisms to engage and activate patients to make behavior changes
- Effective support programs for patients while making these changes
Payment models must support SBDoH
Most provider organizations can’t afford to build comprehensive services that support behavioral determinants of health unless payers are willing to move to value-based insurance design. Fee-for-service (FFS) reimbursement approaches are not designed to offer the necessary financial incentives for providers to address behaviors with preventive-oriented care. Organizations that have built comprehensive patient-centered services that address medical, social, behavioral, and mental health issues know that this wholistic, preemptive approach to health isn’t sustainable without adequate reimbursement.
As the payer survey referenced in the beginning of this blog showed, most payers are moving toward patient-centric approaches that incorporate SDoH. The next step is arming providers and support teams with the application of socio-behavioral data into the caregiving process. This can be achieved by aligning payment incentives that supply the care team and referral partners with the right resources to facilitate proactive interventions.
Value-based insurance design
Value-based insurance design, where payers establish incentives for preventive care and healthier behaviors, can provide the financial incentives to pay for upstream, behaviorally-oriented interventions. For example, payers can incentivize patients to stop smoking, or eliminate co-pays for yearly physicals and age-appropriate health screenings. They can also influence how, where and when providers deliver care through bundled payments, bonus payments, and capitation to support providers in caring for the whole patient rather than being reimbursed for stand-alone services.[9]
When treating high-cost patients with chronic conditions, the right financial incentives allow them to create more long-term, holistic care by partnering with resources outside the traditional care setting (e.g., nutrition, mental health, and even ride services such as Uber or Lyft).
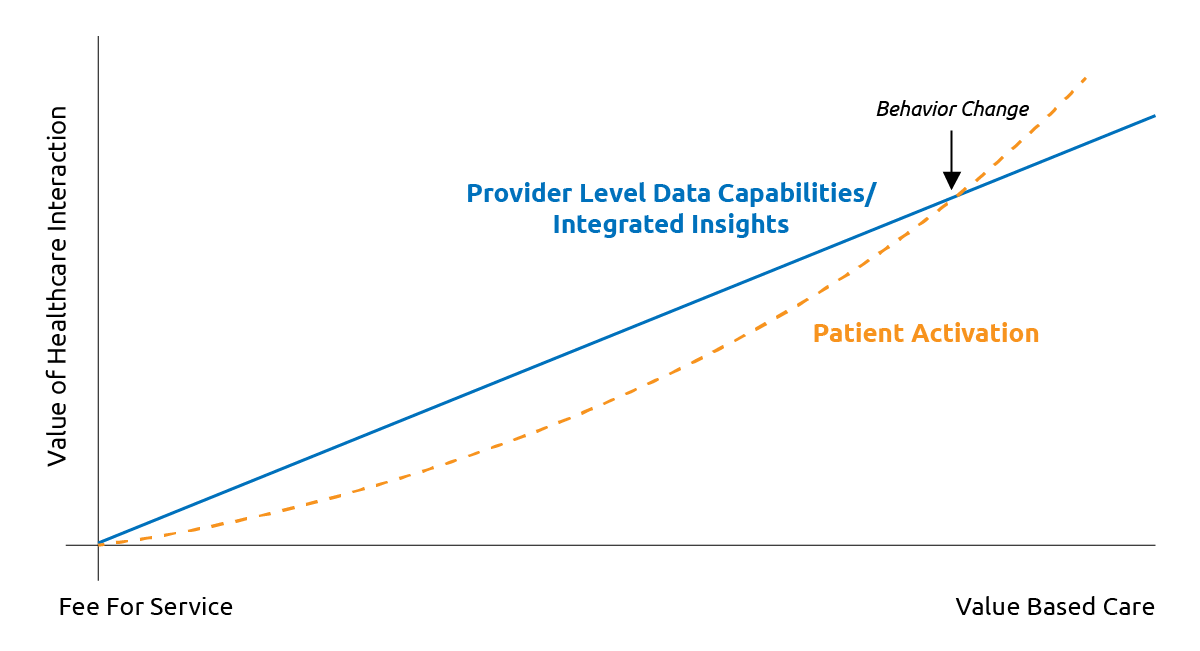
Figure 3: Behavior change is more likely to occur when payment models incentivize providers to gather and act on SBDoH data.
Payers are crucial to this process. Without reimbursement models that encourage a comprehensive care approach rather than the downstream, episodic approach we’ve had under FFS, providers and referral partners will struggle to afford delivering proactive care. Payment models that incentivize gathering and acting on SBDoH information will empower providers to activate patients to healthier behaviors.
Read our white paper, Zip Codes Alone Don’t Deliver, for a more in-depth look at SBDoH, including real-world examples of how it can be used by healthcare providers, payers and other organizations.